It was my father who alerted me about the “white lives matter” protest scheduled today in Huntington Beach, California.
“I’m so glad you don’t live there anymore,” I sighed. We both knew that this protest would likely occur around Pacific Coast Highway and Main Street, an intersection we had crossed hundreds of times in our lives. When I was a child, each parent grasped one of my hands and ushered me across PCH to access the famous Huntington Beach pier. As a youth, I rode my Schwinn 10-speed bicycle underneath the pier, usually my father ahead of me and my mother behind me. As a younger adult, the three of us walked to the end of the pier, where my parents had scattered the ashes of my paternal grandparents. Six months after my mother died, my father and I, along with a few other distant relatives, scattered her ashes into the rolling waves.
In high school, I learned to avoid the pier after dusk because skinheads were often around Main Street. At the time, I did not fully understand their beliefs nor the danger they represented. Now, as I read about the recent KKK propaganda and white supremacy violence from the years I lived there, I wonder how much racism we experienced during my youth that neither my parents nor I recognized. There was (and is) great pressure to assimilate. For many years, I attributed my discomfort to personal defects. Perhaps ignorance is bliss: Had I recognized and acknowledged the atmosphere of white supremacy, would I have done anything different? Could I have done anything differently?
The pandemic has forced us all to view everything through a different perspective. We recently got a microscope in an effort to offset the crushing psychological weight of illness, isolation, suffering, and death. The microscope also forces a different perspective.
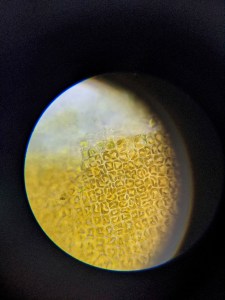
Here’s an image of fresh seaweed from Puget Sound (400x):
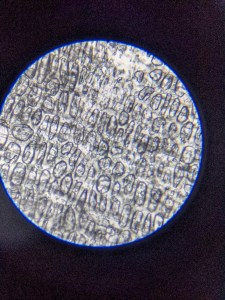
Here’s an image of garlic skin (100x):
Plant cells continue to build organized structures; chlorophyll continues to convert sunlight into sugars; carbon continues to cycle in and out of life forms. The seasons will continue to change; this season of grief, loss, and sadness will also pass.


