I wasn’t familiar with StoryCorps until I received an invitation to record with them. They were looking for people who were front-line workers during the Covid-19 pandemic. Once I learned that the recording would be archived in the Library of Congress, I signed up.
I still believe that most people don’t want to hear anything about the pandemic. Prior to the recording, I have said little about it. (My conversation partner in the recording has been a close friend of mine for over 20 years. Almost everything I shared during our recording she had never heard before.)
There was a time when I literally could not say anything about it: my mind would go blank, my chest would tighten, and no speech would come out.
“I don’t know,” I’d finally say. The blankness—how expansive it was, how it encompassed everything—was overwhelming.
I myself have not listened to the recording and don’t expect that I will anytime soon. Even though the recording was nearly an hour, it still wasn’t enough time. (Enough time for what?) Working as the medical director during the pandemic was the hardest thing I’ve ever done in my professional career. I am thankful that I was given the chance to talk about it.
If one person, 100 years from now, before, during, or after another pandemic, benefits from hearing my experiences, then it will have been worth it. May they learn from my experiences and errors.
I don’t remember these from my youth, though they seem to happen most years now on the West Coast.
An atmospheric river that reaches Seattle is often called a “pineapple express” because the long band of moisture in the atmosphere originates around Hawaii. When the pineapple express arrives, the temperatures here become unseasonably warm (mid to high 50s°F / 12 to 15°C) as the rain falls.
The thing about rain in Seattle is that it usually isn’t rain. It’s more like a mist, a quiet visitor that stops by maybe for an hour or two, then slips away. Within the hour the drizzle returns again, just to make sure you didn’t forget about it. This is why most people here don’t use umbrellas. Raincoats are enough; umbrellas are a burden.
In contrast, the rain of atmospheric rivers demands your attention. The droplets are heavy and full. The water falls in sheets. It’s the mob of young people dressed up like Santa who sing Christmas carols off-key on a crowded light rail platform.
A particularly long river in the sky recently passed above Washington State. Grey clouds rushed overhead, churning past each other like currents of a river, dark water soaring through the heavens. Mud slid, highways collapsed, and lakes formed.
Walking around in it was like walking through a warm blizzard: My face stung from all the water droplets slapping against my cheeks. I had to squint to keep the water out. One afternoon, despite only walking for about 30 minutes, the hems of my pants were soon dragging on the ground. The rain had penetrated every thread and the weight of the water stretched everything down.
There is a small city in South King County that operates its own jail. It has only around 100 beds. (Compare this to the main county jail, which operates two adult facilities with around 1500 beds.)
This small city jail is near one of the rivers whose levee failed. Even as of this writing, the major roads on three sides of the jail are closed, one of which is a state highway. At the height of flooding, the state ordered people to evacuate.
What do jails do when the state orders people to evacuate because of a flood?
Reputable word on the street is that this jail took two actions:
Some people were released from jail. I don’t know what system jail officials used to determine who should be released. Presumably there was some consideration about the severity of the alleged crime. Releasing people from jail, though, results in the former inmates themselves holding the hot potatoes: If people have been ordered to evacuate and roads are closed, how do they return to their homes? (What if they don’t have homes?) People leave jail with only the belongings they came in with (and sometimes not even that), so if they didn’t come in with rain gear, oh well.
Other people were sent to a jail on the other side of the Cascade Mountains. This means inmates piled into secured vans or buses and travelled about 150 miles to Central Washington. Again, I don’t know what system jail officials used to determine who to relocate. Jails are meant to serve the local community and people can be released from jail unexpectedly. Will these people get a ride back to this small city? Will they have to figure out their own way back? With the exit of the atmospheric river, a polar vortex has taken its place. There is snow on the pass.
May our federal government stop manufacturing artificial disasters through inhumane policies. Natural disasters are distressing enough.
For those of you who don’t follow baseball, the Seattle Mariners were in the running to go to the finals in baseball, called the World Series. (So American, of course, to call the finals the “World Series” when it doesn’t involve the entire world!) The Mariners are the only team in all of Major League Baseball that has never been to the World Series.
As such, you can imagine how much of a frenzy the city was in. The Mariners flag was hoisted to the top of the Space Needle twice! The downtown skyscrapers coordinated their night lights to glow in Mariners colors. The mayor raised the Mariners’ flag at City Hall.
Game 7 in the semi-finals, which happened last week, was the “win and go to the World Series, or lose and go home” game. The Seattle Mariners lost.
Over the past week, since that loss, the city has been distraught.
Immediately following game 7, there were brutal postgame interviews. Sports journalists, for obtuse reasons, asked weeping baseball players how they felt.
Here’s Cal Raleigh, our inimitable catcher, showing what his face looked like when he was seven years old and heartbroken:
See how he ran his hand through his hair? That was a desperate act of self-soothing while multiple cameras gave him no place to hide his flushed face and wet eyes.
Meanwhile, here’s Bryan Woo, who turned out to be the team’s ace pitcher this year. He’s not crying, but he is also just trying to get through the interview. A wail of despair interrupts him:
The man whose heartache was heard, but not seen, was our cool center fielder, Julio Rodriguez.
So, are grown men allowed to cry or not? Here were professional athletes caught in the throes of disappointment and sadness. They were crying. Sports journalists pushed microphones into their faces and asked them how they were feeling.
On the one hand, I appreciate this exercise: It’s a chance for these robust young men to model (to other males) how to use words to describe internal experiences. They’re not smashing bats into the walls or punching the journalists. You can talk about unpleasant emotions without resorting to violence or destruction.
On the other hand, asking people about their feelings on camera when they are obviously distressed seems unkind. Sure, baseball players, as public figures, have training about and responsibilities to the media. But such pointed questions do nothing to soothe or support the person. Reporters can also learn the exact same information — how do you feel about losing the biggest game of your professional career to date? — an hour later, when people have had the chance to cry and wail in private. Show some respect, give people some dignity!
But we apparently want to see our heroes cry. We want to know that they feel just as sad as we do.
There are many other people throughout the nation who are crying. They are not professional baseball players; they are not famous. Many of us will never know any of their names.
Some of them were looking forward to leaving the street and moving into an apartment! With winter right around the corner, the anticipation of living somewhere dry and warm was thrilling. Because of the government shutdown, though, the mainstream vouchers that would have paid for those apartments are invalid. So they will have to wait for the government to open before they can move inside.
Many of these same people have Medicaid for health insurance. There are also millions of other people with Medicaid who do know where they will sleep tonight.
The federal government has somehow concluded that it’s not worth it to spend money on health insurance for poor people. But, it is somehow cool to take that money to give tax cuts to people who are wealthy. Yes, it is true that, one day, we will all die. Taking health insurance away from poor people, though, is spiteful. It only makes it more likely that they will needlessly suffer while they are alive.
You know what makes suffering worse? Hunger.
The government shutdown, if not resolved by November 1st, will also shut down the Supplemental Nutrition Assistance Program (SNAP). This program, also called “food stamps”, gives financial aid to poor people to help them buy nutritious food. Food banks are already struggling to provide enough food to visitors. Furthermore, here in Washington State, many grocery stores have closed.
Some people are already hungry. More people will join them.
Yes, you’re reading this right: Soon, the same group of people will have increasing struggles to access food, health care, AND housing. What they all have in common is poverty. Literally no one ever says, “When I grow up, I want to be poor and rely on welfare!” Being poor is not a moral failing. No one, regardless of how much money they have, deserves to have the foundations of wellbeing — food, shelter, and health — taken from them.
But we apparently don’t want to see poor people cry. We don’t want to know their sadness. Some people think poor people deserve to be sad. Others think that poor people are not people.
What would we have to admit to ourselves if we felt their sadness? What would we have to change if we acknowledged that their sadness is real?
In January of 2024, I made a deliberate choice to be a Baseball Fan. There were two reasons behind this:
My spouse is a lifelong baseball fan and I wanted to be a better spouse. We had gone to a few games when his team was in town to play the Seattle Mariners, but my appreciation was limited to “vibes” only.
Someone I loved very much was disintegrating. Cheering a baseball team was a socially acceptable way to shout and channel my heartache in public.
I had choices to make, though: Do I invest my enthusiasm in my spouse’s team? In their pinstripes they have won the most number of World Series (and reminds everyone of it). Or do I dedicate my ardor to the team that has never been to the World Series, the Seattle Mariners?
Dear reader, you already know who got my vote. The West Coast is the Best Coast.
A sponge for learning, I asked many questions during my 2024 baseball education. Once I understood what “starting rotation” meant, what made the Mariner pitchers so effective? Why does “Wins Above Replacement” matter? What does “On-base Plus Slugging” represent? Why did Ty France get hit by pitch so much? Teams can designate players for assignment just like that???
My spouse’s eyes never rolled out of his head, though that would have been a reasonable response to some of my questions. Every morning I read the SB Nation site for the Mariners, Lookout Landing. I announced my burgeoning interest in baseball to other Mariners fans. They all looked at me with some amount of pity.
In our 2024 Christmas card I commented that my choice to become a fan of the Seattle Mariners was a mistake. I now understood the shirt I had seen around town: A trident, to represent the Mariners, and the text, “Maybe next year!“
Before the baseball season started in 2025, the person I loved very much died. As the year unfolded, wars continued, injustice ascended, ethics eroded. Cheering a baseball team is a socially acceptable way to redirect the energies of grief and anger in public.
My investment in the Seattle Mariners grew. This culminated in the sheer amount of kilojoules I spent this week on this team, which is now the American League West champion! This hasn’t happened in 24 years.
Furthermore, our humble catcher, Cal Raleigh, made home run history, both as a catcher and as a switch hitter. (His nickname is “The Big Dumper”. Have you seen the size of his butt?)
This has prompted questions about identity:
I didn’t grow up in a baseball household. (Basketball came first, then football.)
I historically have found baseball boring.
Could fans of America’s pastime look like me?
Am I now one of those people who can spout random facts about baseball?
Dear reader, the answer to all those questions is yes. That’s super weird.
As the Seattle Mariners crested towards the end of the season, baseball became a laboratory of communication.
I previously envied the way men who did not know each other could immediately engage in energetic conversations about sports. Sometimes it seemed like they had known each other for years.
What I noticed now, though, was the increasing amount of communication — particularly in the form of text messages — solely about baseball. Practically all these people are good friends I have known for years. There are real tragedies happening in their lives: parents who are deteriorating; pets dying; friends with conditions that elude treatment; people losing their jobs.
Meanwhile, they send messages acknowledging Cal Raleigh’s 60th home run.
How are they themselves doing? No comment.
I don’t know if it’s true that, because of my professional training, it is easier for me to have in-depth conversations with people. Do I have skills to create conditions so people will be more likely to share sensitive personal information with me? I hope so, but I don’t actually know.
It’s true: Talking about baseball is easier than talking about hopes, fears, dreams, and loss. It’s natural to avoid delving into more meaningful topics. We fear how others will react to our vulnerabilities, to the soft spots we keep covered to prevent bruises from the outside world.
The thing is, we’re often our own harshest critics. Our good friends aren’t umpires. They’re not calling balls and strikes on us. They are instead in the dugout or on deck, admiring our approaches to the plate.
But let me be honest: Have I already forgotten the reasons why I chose to become a Baseball Fan? Weren’t there thoughts and emotions I sought to shun? I couldn’t escape anticipatory grief. The crying was exhausting. Wasn’t I looking for a healthy yet avoidant way to cope?
So, here’s to the 2025 Seattle Mariners. May their success continue. May they go to (and win!) the World Series. May they continue to be a bright spot amid the challenges we all have in our small lives and big communities.
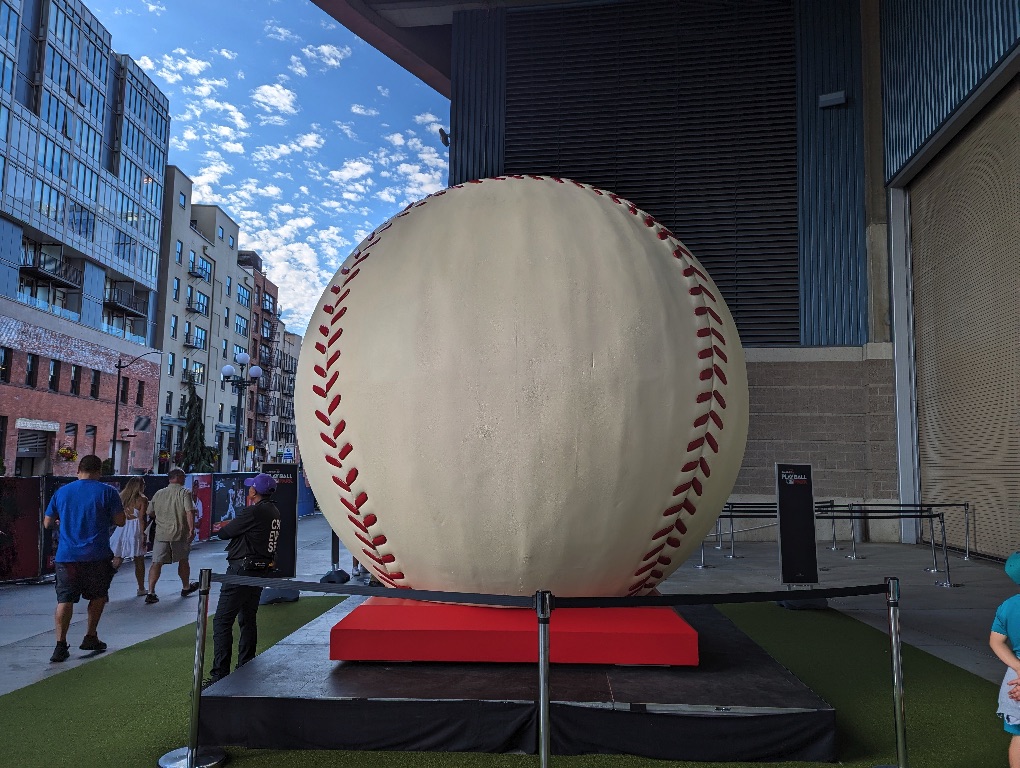
For those of you who read my last post, I have an update: I saw the World’s Largest Baseball!
In addition to sharing my impressions about this artifact, I will also shout into space my opinions about Play Ball Park, where the World’s Largest Baseball currently resides. (Important context: Because this giant ball was in the free portion of Play Ball Park, that is the only part of the park I visited.)
Access. I will, no doubt, go on for way too long about access to Play Ball Park. (This is an excellent example of attentional bias. Because of the work I do, I am often thinking who can and cannot access care. I regret to inform you that I am now going to carry on about access to the World’s Largest Baseball.)
In order to enter Play Ball Park, you must download an app so you can show a QR code on your phone to the gatekeepers.
What if you don’t have a smartphone?
What if you don’t have a robust data plan with your cell phone carrier? (MLB does not provide clear orientation about how you must have this app. A lot of people who wanted to enter the park ended up loitering outside the gate to download the app and complete the questionnaire—more on that in a moment. If MLB made it crystal clear on its website that you need this app to access any part of the park, even the free portion, people could have gotten this app somewhere with WiFi.)
The app asks for your name, date of birth, home address, and contact information. Sure, you can lie, but I’m just speaking to the principle here. Why does MLB need to know this information? (You and I both know why, but just indulge me.) Must I share this data when I just want to see a giant baseball? (I’m turning into that Old Person who is paranoid about sharing personal information… even though I maintain a blog that allows me to shout into space.)
To be fair, most, if not all, people who go to Play Ball Park have a smartphone. And most people in this area have home internet access (per the US Census, over 93% of King County households have a subscription to broadband internet), so most are familiar with apps and their data-gathering ways.
The World’s Largest Baseball is not a true baseball. It has a diameter of 12 feet and there are numerous autographs from baseball luminaries on one side. (The photo accompanying this post shows the “back” of the baseball.) Guests are not permitted to touch the baseball or sit on the base. It looks like it is made of metal or other hard material. The red stitching appears to be plastic bumps that are attached to the surface. The panel on the “side” of the ball is secured with bolts and nuts that are painted baseball white. The ball does not appear to be a complete sphere; it looks like the bottom of the ball is flat so it sits flush inside the red base.
Even though the World’s Largest Baseball is a fraud, I still took a photo with it. Who knows when I will see an enormous fake baseball again?
The Budweiser Clydesdales were in cages. They are large horses. I don’t know if they ever come out during park hours. Few people were looking at them. This entire situation made me sad.
Fake ball, real smiles? (Julio was the only cutout who was smiling.)
There was a significant police presence in and around Play Ball Park. David Gutman with the Seattle Times wrote a thoughtful piece about the “two Seattles on display as thousands attend MLB All-Star festivities” that has relevance here. Seattle Police was out on foot, on bikes, and in vehicles. It’s been a long time since I’ve seen so many law enforcement officers; it’s not often that we’re surrounded by so many people carrying lethal weapons. It’s not that I felt more or less safe; it was just unsettling to see the amount of firepower amidst a sea of baseball jerseys.
The trains were packed this afternoon for the Home Run Derby. For a few moments, I was transported back to the New York City subways: Standing room only, holding onto poles and straps in awkward angles, and taking shallow breaths to cope with body and breath odors. However, people here were only passive-aggressive (“it would be nice if people moved down more”) versus just plain aggressive (“MOVE, PEOPLE”). I did not need to throw my elbows to escape the train when I got to my stop.