Dear reader, what do you suggest I talk about during a presentation about homelessness and mental illness?
I’ve been invited to talk to a small class at the large local university about homelessness and mental illness. The overall course is about homelessness (I think) and the students apparently range from undergraduates to medical students to faculty. It sounds like it’s one of those seminar courses that is not required for anyone, which means that the students presumably have an active interest in this topic and want to be there.
It seems that an introductory overview, 101-level talk might make the most sense, but I only have one hour and this topic is vast. While I always do my best to make statistics and data interesting, I don’t know that rattling off percentages is the best use of time. Anecdotes and cases are compelling, though I worry about missing larger points about the intersection of homelessness and mental illness.
Some of you have been reading my writing online for years (decades?–thank you for the gift of your attention!) and some of you have not, though I get the sense that most of you have some interest in psychiatry and homelessness. If we work with the assumption that this class has similar interests as yours, what do you suggest I talk about? What would be most interesting or compelling to you about the topic of homelessness and mental illness? If I’ve written something here in the past on this topic that you found useful and could share in this class, could you let me know?
It’s been years since I’ve opened comments on my blog (due to spam comments and some veiled death threats), but it’s a new year and I would like to learn from you. Please leave a comment below with your advice and suggestions. Thank you!
Happy Lunar New Year! May the Year of the Rabbit bring you health, wealth, and peace. I send specific wishes of safety and serenity to those who are afflicted by war. Some cultures believe that there is a rabbit in or on the moon. I hope that those who are living through war know that, when they look at the (rabbit on the) moon, there are other people on the planet who are also looking at the moon and pray for them.
What to Do If a Rat Comes Up Your Toilet. This is actual guidance (in cartoon form!) from the Seattle-King County Public Health Department. Some regions have experienced flooding due to the rivers of rain running through the sky. May you never have to deal with this problem, but if you do, now you know how to proceed.
“If a body sinks and decomposes underwater, scavengers begin feasting — often picking at the soft ligaments and connective tissues of human ankles first, causing the feet to become separated.”
“Changes in sneaker design since 2007 have made shoes more buoyant, as manufacturers began using lighter foam for soles.”
“Since 2007, nearly two dozen human feet in sneakers have washed up along the coasts of the Salish Sea in the U.S. and Canada.”
It is a travesty of justice that law enforcement agencies need “to crowdfund or seek donations from philanthropists” to help identify a deceased person.
The Enduring, Invisible Power of Blond. The incisive and provocative Tressie McMillan Cottom wrote this piece that ostensibly is about the power of blondness; the key quote is this: “When people have outsize emotional reactions to benign inquiries about their self-evident beliefs, it is often an indicator that status is doing invisible work.” Though there are some loud, public pushes to encourage (or cajole or threaten or berate) people to recognize their prejudices and change their behaviors, meaningful shifts actually result from quiet, internal effort. Recognizing and reflecting on “outside emotional reactions” are opportunities, as some say, “to do the work”.
Recommended: Dr. Bill Gardner’s Substack. I first started reading Dr. Gardner’s writing many years ago on the health services blog, The Incidental Economist. He now shares his thoughtful wisdom on I Have Serious News…. Much of his current writing focuses on his cancer diagnosis. He continues to write with clarity, compassion, and insight. If you seek inspiration about clear communication about health, both on individual and population levels, consider subscribing to his Substack.
Items related to systems of health care that I learned and thought about this week:
National Medical Association. I am embarrassed to confess that, nearly 20 years after graduating from medical school, I learned only this week about the National Medical Association. This came about while I was learning some of the history of the American Medical Association (AMA). In short, the National Medical Association was created because the AMA would not admit Black physicians into the organization. (I have never been a member of the AMA. My reasons have been squishy; I never truly believed that the AMA represented me or my interests. That hasn’t stopped the AMA from sending me invitations in the mail to join! It seems that over 80% of physicians are not AMA members, so I’m certainly not alone.)
Alexander Graham Bell and Eugenics. This Journal of the American Medical Association(emphasis mine) editorial from 1908 reports:
The subject of the production of better men and women was brought before the American Breeders’ Association by Professor Alexander Graham Bell, the inventor of the telephone, who for many years has been interested in certain social questions, especially those relating to the condition of the deaf and the result on the next generation of the consanguinity of parents as regards the production of deaf and blind children.
No one ever brought this up when we learned that he invented the telephone.
It appears that Bell’s interest in “breeding” was his observation, though the collection of some statistics, that parents who are related to each other seem more likely to bear children who are deaf. Bell made “an appeal for the collection of statistics by trained men who are interested and who have the opportunity to secure the definite detailed information” related to “the production of better children”. The unnamed author(s) of the editorial go on:
We are securing survivals to a much greater degree than before, and now it becomes a duty to secure, so far as it is possible, the origin of members of the race who will be worthy of survival. After all, the most important problem in evolution is not so much the survival of the fittest as the origin of the fittest.
Over 100 years have passed and this ugly question of “breeding” persists.
The Chinese Exclusion Act. I’ve commented on this Act before (here and here), but here’s an opportunity to pile on the AMA even more. In 1901, the Journal of the American Medical Association published a “minor comment” about “The Exclusion of the Chinese“, which you can view in its entirety in the link above.
Reading this made me think of vile rhetoric that has revived during this Covid-19 pandemic. Recall recent references to “disregard of sanitation” due to “[maintainence] to the fullest extent their oriental habits and traditions”. The Chinese, they just won’t do as we do.
“That this is a Christian country and we regard them as heathen, should not make us altruistic to our harm.”
Prescriptive Authority for Psychologists. There is a House bill in the Washington State Legislature that will give prescriptive authority to psychologists. Five US states currently allow psychologists to prescribe medications.
While it is easy to stumble into a debate about whether this should happen or not, I think this is a distraction. This debate is a manifestation of failure in public health policy.
Instead of trying to increase the number of people who can perform a highly specialized task, why not increase the availability of community supports and services so people don’t need highly specialized treatment?
Consider the decrease in anxiety and depression that would result if people were confident they could pay their rent? feed their families? take time off to care for their newborn? secure an education or training–whether college or vocational school–that supports stable employment?
Think of the decrease in stress and trauma if people had better options than to sell drugs or sex? if neighborhoods had more green spaces and less air and noise pollution? if they had adequate and essential protections as “essential” workers?
Medical Mistrust and Meeting People Where They Are At. This paper about medical mistrust, racism, and health prevention describes an elegant way to recruit study participants: “collection of data [occurred] primarily in barbershops, venues with documented recent success in reducing blood pressure in African-American men”. It is elegant because it is simple, effective, and successful.
When I read this, I recalled a suggestion my father had around the time the Covid-19 vaccines were released. He lives near several Asian grocers, many of which are more like bodegas than grocery stores.
“Why don’t they set up vaccination stations outside these grocery stores? Everyone needs to eat. Elderly people go to these stores all the time. Laborers get snacks and cigarettes. Make it easy for people.”
Sometimes (often?) the best and most effective health care happens outside of medical spaces.
A belated winter gift for readers: Here are some articles and other media I have found useful and interesting in the past few months, which you may enjoy, too.
Still Processing. This is a podcast from the New York Times. “Wesley Morris and J Wortham are working it out in this show about culture. That means television, film, books, music — but also the culture of work, dating, the internet and how those fit together.” Wesley Morris is a superb writer, too, and has the Pulitzer Prizes—plural! 2012 and 2021!—to prove it.
Lucas Sin. He is a chef who is from Hong Kong and now works in New York. He seems thoughtful, communicates well, and has an understated enthusiasm for his craft.
Mystery Menu. Sohla and Ham are both chefs. Not only do they have expertise in creating dishes from strange ingredients, but they also seem like delightful people.
Building Resilient Organizations. Maurice Mitchell’s analysis of dynamics in progressive organizations is intelligent, incisive, and inspiring. (There are similarities with ideas in John McWhorter‘s writings. I learned about Mr. Mitchell through Chris Hayes.)
Escaping American tribalism: Only personal bravery can end polarisation. William Deresiewicz, like other writers I admire, shares sharp, provocative opinions and insights (“You change your mind when you consent to stop ignoring things you know full well but do not want to think about”). I look forward to reading his most recent book, The End of Solitude: Selected Essays on Culture and Society.
Glass Onion: A Knives Out Mystery. As someone who has read nearly all of Agatha Christie’s novels, it is delightful to see Hercule Poirot reincarnated as Benoit Blanc. It’s a fun movie. (And Edward Norton and Janelle Monáe make such gorgeous eye candy!)
A few questions I have asked ChatGPT, the artificial intelligence chatbot:
“Is the journalist Chris Hayes actually a donut?”
For reasons that make sense to no one except for me, Chris Hayes‘s face reminds me of a donut: round, smooth, and fluffy. (Maybe this is just an inappropriate way to comment that he has nice skin?) I appreciate that ChatGPT not only wonders why I think he is a pastry, but also makes it clear that Chris Hayes is not a donut.
“Which is better: left turns or pizza?”
ChatGPT has no patience for my foolishness, though graciously explains that left turns and pizza are categorically different things. I appreciate ChatGPT deferring to my personal preferences and experiences. (If I had to choose for only one to exist, I think I would choose pizza. Three right turns make a left turn, but other flatbreads are not pizza.)
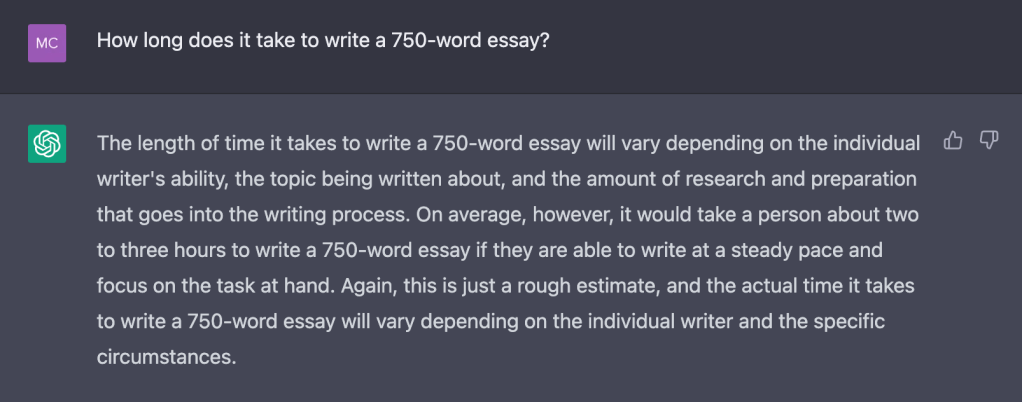
“How long does it take to write a 750-word essay?”
I found this response validating. I have wondered if I’m just slow, as it often takes me a few hours to write a post for publication here. Those few hours of writing transform into a mere three minutes of reading!
And that, dear reader, is how I have “cheated” in generating this week’s blog post.