
This TikTok video provides an accurate (and shouty) summary of the National Guard member who leaked classified military documents. In short, it appears that the Airman shared these documents in an effort to elevate his status within an online cohort. (Someone on the internet opined something like, “This was a cosmic level of stepping on a rake that hits you in the face.” Correct.)
We all have engaged in behaviors to heighten our position in relation to others. Depending on who you ask, some argue that we are constantly adjusting our behaviors to communicate and maximize our status.
Our perception of our own status is not always accurate. It seems that we sometimes exert tremendous effort to demonstrate high status to make ourselves feel better, rather than to assert that we have higher rank than others. (Much research has been done to show how humans assess and react to status.)
Maybe it’s a stretch to link demoralization and status to each other, though this is what has come to my mind over the past few weeks. Demoralization is usually framed as an individual process, whereas status involves groups of people.
Merriam-Webster provides the following definitions:
- demoralization: weakened morale; to be discouraged or dispirited
- status: position or rank in relation to others
I’ve written about demoralization before, though it was more in reference to individuals experiencing medical illness. The paper I reference in that post offers this definition of demoralization:
the “various degrees of helplessness, hopelessness, confusion, and subjective incompetence” that people feel when sensing that they are failing their own or others’ expectations for coping with life’s adversities. Rather than coping, they struggle to survive.
This is where I might be speaking out of turn: Is it fair to apply principles usually applied to a single person, particularly one’s intrapsychic processes, to groups of people? (Would I be a true psychiatrist if I didn’t use the word “intrapsychic“?)
But let’s consider this together. I’m starting with the Airman, but that isn’t actually the point of this post.
What if that Airman was feeling demoralized? Within his Discord group, he may have been able to rely on his age to maintain high status. What teenager doesn’t think a 21 year-old person is cool? But what if group dynamics shifted and, suddenly, the Airman was no longer the proverbial “alpha”, but had been demoted to a “beta”?
In an effort to restore his status, he might have employed any one of the strategies to reduce his vulnerability:
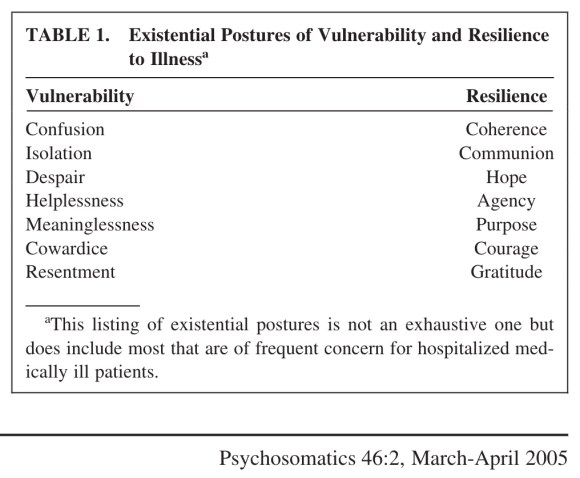
The sharing of classified military documents isn’t a demonstration of resilience, but it is a display of power that produces postures of coherence, agency, and courage. In sharing classified papers that only he has access to, he is dissolving any confusion he or anyone else may have about his “rightful” status. To combat feelings of helplessness, he demonstrated agency to provide evidence of his power. It takes some flavor of courage (…) to share sensitive information. By sharing these documents with his Discord cohort, he facilitated communion, established a purpose for himself, and got to bask in the gratitude of his friends. What a way to escape the isolation that accompanies a degradation of status!
So let’s consider other things that are happening in the nation that might be reactions to demoralization and efforts to reinstate high status: states banning TikTok, banning abortions at six weeks, protecting access to transgender care.
Again, is it fair to apply individual, intrapsychic processes to groups of people, particularly groups of people in politics? (But aren’t political groups comprised of individual people?)
The passage of laws—something that feels real and concrete—brings coherence and fosters communion! It brings hope and purpose! Doing something—exhibiting agency—summons courage and generates gratitude! Your rank in relation to others feels like it is rising. Even though there are people who will view your actions as further erosion of your status, it doesn’t matter: You feel better. You feel more power.
The passage of laws reduces confusion, despair, and helplessness. Instead of feeling isolated, people can channel their feelings of helplessness and resentment into doing something, which makes cowardice evaporate. You may already possess high status—all the other people around you may already defer to you because they view themselves as having lower status. And, yet, if you feel demoralized, the positive regard from others may be insufficient to elevate your own status in your own eyes.
We can never get away from ourselves.




